24 Hours into the Beef Stock Making…
Posted: October 5, 2009 Filed under: Food and it's Impact on Our Health, In The Kitchen with Millie- How To's Leave a commentThe huge bones are simmering on the stove..I felt like a cave woman in my kitchen last night…browning huge beef shank bones in my Dutch oven, in luscious coconut oil. So tonight it has been sloowly bubbling for 24 hours..I added carrots, onions, celery..all organic, with bay leaves, crushed peppercorns…Celtic salt.
And as I just tasted it for the first time…I realized that I have never tasted a true beef stock before…the mouth feel is nothing like the insipid, salty stuff I have had. The grass fed beef is heavenly to cook with…amazingly nutritious. The gelatin is developing, it’s silky texture is amazingly satisfying.
Another 24 hours to go…the house smells amazing.
I’m making beet salad from beets I grew, then roasted with the beef bones in the oven last night. I added dill and rice vinegar, light salt. Mmmm
While it’s bubbling….I’m making a flourless chocolate cake. Here’s the recipe;
Flourless Chocolate Cake Topped with Raspberries

- 12 oz semisweet chocolate chips
- 1/2 cup butter
- 1/4 cup sugar
- 1/4 cup water
- 1 teaspoon instant coffee granules
- 3 eggs
Preheat the oven to 425 F.
Butter the bottom and sides of a 9 inch pie plate.
Place a 12 inch square sheet of waxed paper in the plate and butter the waxed paper.
In a medium sized saucepan, combine the chocolate chips, 1/2 cup butter, sugar, water, and coffee granules. Heat over medium heat for 2 to 3 minutes, until the chocolate and butter are melted, stirring constantly.
Remove from the heat and stir in the eggs until the mixture is smooth. Pour into the waxed paper-lined pie plate. Bake for 10 minutes; the cake will not be completely set in the middle. Cool, cover loosely, then chill for 6 to 8 hours, or overnight.
When ready to serve, remove the cake from the refrigerator and allow to sit for 10 minutes. Invert the cake onto a large flat serving dish and remove the waxed paper.
Top with raspberries across the whole top, begin in the middle and work out…letting the raspberry tips straight up.
![]()
![]()
![]()
Virgin Coconut Oil from Tropical Traditions…
Posted: October 4, 2009 Filed under: Food and it's Impact on Our Health Leave a comment Close friends of mine began nagging me a few years ago to check out the company that they were getting coconut oil from, Tropical Traditions. They said the thier coconut oil was the best they’d ever had; unprocessed, made by hand, organic… I had only a few years before began researching saturated fats and the role they play in the body, and eating coconut oil…and was pleased with the organic coconut oil I was already eating. Plus, money was tight and I saw no reason to change to a more expensive product…until I went on the site and read about this wonderful product, and began looking into the differences in virgin oils compared to processed oils.
Close friends of mine began nagging me a few years ago to check out the company that they were getting coconut oil from, Tropical Traditions. They said the thier coconut oil was the best they’d ever had; unprocessed, made by hand, organic… I had only a few years before began researching saturated fats and the role they play in the body, and eating coconut oil…and was pleased with the organic coconut oil I was already eating. Plus, money was tight and I saw no reason to change to a more expensive product…until I went on the site and read about this wonderful product, and began looking into the differences in virgin oils compared to processed oils.
About 3 weeks ago my friends told me they were having an awesome sale, half off on coconut cream, so I ordered some of thier virgin oil. They sent me a book on the company, how the coconut oil was handmade and the health benefits of unprocessed virgin oil.
First of all, the service was wonderful, customer service was excellent, I got my order quickly…the coconut oil and the cream were in glass jars, not plastic. The packaging was all cardboard, no Styrofoam, no plastic.
I love it. I like the taste, the coconut cream is amazing…I made Coconut Fudge Sauce and it is to die for! The cream is coconut concentrate, I use it just like I would heavy cream in a recipe.
The oil I cook with, bake with, use on my hair, my face, my legs after shaving… Coconut cream has always been my favorite oil, mixed with olive oil..to make bar soap or shampoo.
They also carry coconut; shredded, chips, flour (WAY lower on the glycemic index than other flours, a dream to bake with and gluten free!), They carry organic unrefined palm oil, sesame, extra virgin olive oil, soaps, grass fed meat, organic foods.
Here is what info from thier website;
Independent laboratory analysis shows this to be one of the highest quality coconut oils on the market, having the highest levels of antioxidants. This enhanced Virgin Coconut Oil is now in the US market under the Tropical Traditions Gold Label brand. It meets our strictest standards to earn this designation. Today when you buy Tropical Traditions Gold Label Virgin Coconut Oil, you are buying the highest quality coconut oil we have to offer, and it is still made by hand and benefiting families in the rural areas of the Philippines where the coconuts grow.

Is Virgin Coconut Oil the healthiest oil on earth?
Read the research here!
Read what Weston Price has to say about Coconut Oil.
Characteristics of Our Gold Label Virgin Coconut Oil
This Tropical Traditions Gold Label Virgin Coconut Oil is a truly unrefined coconut oil. This coconut oil is made on Mt. Banahaw and surrounding areas from organic coconuts. Coconuts are used fresh (within 24-48 hours of harvest) from small family farms on Mt. Banahaw and other rural places in Quezon Province, the coconut capital of the Philippines. Only the highest quality coconuts are hand-picked from each harvest. The volcanic soil of Mt. Banahaw makes these organic coconuts some of the most nutritionally rich coconuts in the world! Testing done in independent laboratories reveals higher levels of phenolic antioxidants than other coconut oils. The fresh coconut meat is shredded (wet milled), and then cold-pressed using the water from inside the coconuts to make coconut milk. The milk is then allowed to sit for about half a day, while the oil naturally separates from the heavier water. The oil is then filtered from the curds (coconut solids). No chemical or high-heat treatment is used, and this oil contains no trans fatty acids. We do NOT mass produce this oil. It is made by families who are coconut farmers using old-fashioned traditional methods that have been used in the Philippines for hundreds of years. Our coconut trees and family producers are certified organic according to strict USDA standards.
Tropical Traditions also has a Referral Program, so if you place an order with them as a first-time customer, please select “Referred by a friend” and in the box that says “How did you hear of us?” enter my sponsor ID number… 5541380. By telling Tropical Traditions that I referred you, you will receive a complimentary copy of the book Virgin Coconut Oil: How it has changed people’s lives and how it can change yours! by Brian and Marianita Shilhavy with your first order! This book is filled with testimonies and research showing how healthy coconut oil is, and it also includes over 85 recipes showing how one can incorporate coconut into their diet.
I am thrilled to have found this product and recommend it highly.
The Beef Bones Adventure…
Posted: October 4, 2009 Filed under: Food and it's Impact on Our Health, In The Kitchen with Millie- How To's 1 Comment I have been happily making chicken stock for quite some time now.. About a year and a half ago, while working at Native Sun, I kept bugging the employees in the meat department about finding me a case of grass fed beef shank bones. Months this went on, to no avail. They said they couldn’t get an answer…then they said no.
I have been happily making chicken stock for quite some time now.. About a year and a half ago, while working at Native Sun, I kept bugging the employees in the meat department about finding me a case of grass fed beef shank bones. Months this went on, to no avail. They said they couldn’t get an answer…then they said no.
I could find them on the internet, but I’ll go to extremes to keep from having something shipped to me..for environmental reasons mainly..but also wanting really fresh bones. The local co-ops want 35. to 50. to join.. What to do? I finally sucked up and went to Whole Foods…whom I certainly don’t trust for lots of reasons, preferring to shop local, not chains..
But a friend called and said she had asked them about the bones and they had them…so I got up the next morning and schlepped all the way out there. and was told they didn’t have them. They apologized and gave me the meat managers card, who would be in the next afternoon. So I waited til then and called, spoke to him and made arrangements to drive out the next afternoon to get them..he would hold them for me.
He didn’t…or rather when I got there, again, the next afternoon in 5 o’clock traffic…he wasn’t there. Seems he had been taken to the hospital for diabetes. Why don’t health food stores teach people how to eat? Classes on nutrition? Anyway, I whine, they look all over, can’t find them. They talked to the store manager, who had them cut 4 the meat off of 3 shanks…a 40 minutes wait…but t5hey did it. While hanging out at the meat counter, I noticed that bison was on sale for 3.99 a POUND. Wow… bought three pounds… Finally heaved the bones out to the car, with help…and at a great price.
The burger I had that night was the best bison burger I’ve ever had, very fresh, perfect. Wow.
And this afternoon I came home and browned, then slow roasted all those shanks and they are gently simmering for the next 2 days..mmmmmmmm.
Beef Stock

about 5 pounds beef shank bones
2 Tablespoons coconut oil
3 pounds meaty rib or neck bones
5 or more quarts cold filtered water
1/2 cup vinegar
3 onions, coarsely chopped
3 carrots, coarsely chopped
several sprigs of fresh thyme, tied together
Heat coconut oil to slightly above medium heat, place shanks bones in oil to brown. Brown on all sides, even the ends of marrow. Then place in a roasting pan, covered, and brown at 325 degrees in the oven for 1 hour.
Place the knuckle and marrow bones in a large pot with vinegar and cover with water. Let stand for one hour.
Place roasted bones the water with them knuckles and stuff. Slowly bring up to a soft simmer and simmer, covered for…the longer the better..up to 72 hours.
Pour the fat out of the roasting pan. Deglaze the roasting pan, add liquid to pot., Add additional water, if necessary, to cover the bones; but the liquid should come no higher than within one inch of the rim of the pot, as the volume expands slightly during cooking. Bring to a boil.
A large amount of scum will come to the top, and it is important to remove this with a spoon. After you have skimmed, reduce heat and add the thyme and crushed peppercorns.
Simmer stock for at least 12 and as long as 72 hours. You will now have a pot of rather repulsive-looking brown liquid containing globs of gelatinous and fatty material. It doesn’t even smell particularly good. But don’t despair. After straining you will have a delicious and nourishing clear broth that forms the basis for many other recipes.
After you have made the stock and reduced it as much as you want, place the pot in the refrigerator and let it cool overnight. All the fat will rise to the top. Boil that fat with twice the amount of water as fat, let it solidify again, and THEN store it in the fridge or freezer. This removes a good amount of the meaty taste, and whatever sediment is in the fat will sink to the bottom of the pot. Use it like you would schmaltz or any other solid fat — especially for frying or in pie crusts!
You can do this with bacon grease, too, although I don’t know why you would want to get RID of bacon flavor!! 🙂
High Cholesterol = Heart Disease — Myth or Truth?
Posted: October 1, 2009 Filed under: Food and it's Impact on Our Health 5 CommentsThe Response-to-Injury Rabbit Never Developed Atherosclerosis — Why Not?

by Chris Masterjohn
From Cholesterol and Health.com
The pop science version of cholesterol goes something like this: when you eat fatty foods, especially foods rich in animal fat, the saturated fat and cholesterol in these foods wind up in your blood and stick to your arteries. Since saturated fats are solid outside your body, they will be solid inside your body too — depsite the 30-degree increase in average temperature. Arteries are much like pipes. When they get caked up with grease, blood flow is impaired, and a heart attack ensues.
None of the prominent scientists who promoted the idea that cholesterol is a critical factor in the development of heart disease ever believed anything remotely resembling this nonsense. From the beginning, they recognized that atherosclerotic plaque accumulates behind the layer of the artery in contact with the blood, called the endothelium, and that the cholesterol and fat within it is engulfed in white blood cells.
The theory these scientists promoted looked something like this: when the cholesterol level in the blood increases, it penetrates the arterial wall and gets stuck; white blood cells circulating in the blood then enter the arterial wall and gobble up the cholesterol; the accumulation of lipid-loaded white blood cells causes local injury, leading to cell death, calcification, and the development of a collagen-laden "fibrous cap" over the atherosclerotic lesion. When the cap ruptures, the blood clots, blocking the artery and causing a heart attack. This is called the lipid hypothesis.
But is this true? Books and web sites devoted to debunking this theory have come out of the woodwork over the last decade; books defending it have followed suit. Consider the following titles to see just how controversial the idea really is:
- The Cholesterol Myths: Exposing the Fallacy That Saturated Fat and Cholesterol Cause Heart Disease by Uffe Ravnskov, MD, PhD (2000).
- The Great Cholesterol Con: Why everything you’ve been told about cholesterol, diet, and heart disease is wrong! by Anthony Colpo (2006).
- The Cholesterol Wars: The Skeptics vs. the Preponderance of the Evidence by Daniel Steinberg, MD, PhD (2007).
- The Great Cholesterol Con: The Truth About What Really Causes Heart Disease and How to Avoid It by Malcolm Kendrick, MD (2007).
So is the theory that cholesterol causes heart disease just a myth? Or are the skeptics truly waging a war against the preponderance of the evidence?
The Cholesterol Debate — What Causes Atherosclerosis?
The truth is that each of these authors makes important points. Were there never any good evidence that cholesterol was involved in heart disease, there would be no National Cholesterol Education Program, no statin empire, and Daniel Steinberg could never have written a book plus over 200 scientific papers on the subject. On the other hand, were there never anything seriously wrong with the mainstream dogma on the issue, Ravnskov, Colpo, Kendrick, and many other authors could never have built their careers around pointing out the gaping holes in the theory.
There is no one cause of "heart disease." "Heart disease" is a heterogeneous compliation of diseases of the heart and blood vessels with many different causes. Some of these include disturbances of the rhythm of the heart, calcification of the middle portion of the blood vessels and calcification of the heart valves, and congestive heart failure. The question I address in this article is whether and in what sense cholesterol is involved in atherosclerosis, the development of fatty and calcified plaques in isolated, raised lesions, which can cause heart attacks by rupturing, clotting, and blocking arteries.
In 1933, the famous proponent of the cholesterol-fed rabbit model Nikolai Anitschkov declared that atherosclerosis had been shown to be of an "infiltrative" character rather than a "degenerative" character and was driven by lipids (fatty substances) rather than by inflammation. He did not deny inflammation was involved, but believed that it was secondary to lipid infiltration. Many opponents continue to claim that the root cause driving heart disease has nothing to do with lipids and everything to do with inflammation and that it is degenerative rather than infiltrative in character.
As we will see below, these are all correct! Atherosclerosis is largely driven by the degeneration of lipids which infiltrate the blood vessel and thereby cause inflammation. Inflammation from other sources may accelerate the process or further the degeneration of the atherosclerotic plaques once they are formed, but the initiating factor for fatty plaques appears to be the degeneration of lipids — especially the degeneration of polyunsaturated fatty acids (PUFA).
In order to begin looking at the evidence, we must go back a century in time to the cholesterol-fed rabbit. The cholesterol-fed rabbit model came on the heels of extensive investigations into what would later be termed the "response-to-injury hypothesis."
The Response-to-Injury Rabbit Model
Around the turn of the twentieth century, research into the cause or causes of heart disease was in full throttle. A 1933 compilation edited by E.V. Cowdry entitled Arteriosclerosis: A Survey of the Problem (New York: Macmillan) contained twenty reviews of investigations into the matter, including statistical relationships, the distribution of the disease in wild animals, the distribution in humans according to race and climate, nutritional influences, the physical and chemical nature of the changes that occur in atherosclerotic tissues, and experimental models of the disease.
Nikolai Anitschkov, who developed the cholesterol-fed rabbit model, wrote the 50-page review of experimental animal models.1 Much of this research was published in German, so Anitschkov’s review is an invaluable resource.
According to Anitschkov, early ideas about the origin of arteriosclerosis — a general term for hardening and damage to the arteries, of which atherosclerosis is a specific type — saw the diseases as a response to injury. The injury was primarily seen as either a mechanical or a toxic factor, and was sometimes believed to be injury to the nerves rather than injury to the blood vessels. Researchers carried out a multitude of experiments on rabbits and other animals, including the following:
- Mechanical damage to the blood vessels including ligating, pulling, pinching, and wounding them, and cauterizing them with galvanic wire or silver nitrate.
- Increasing blood pressure by constricting the blood supply through the aorta, damaging the kidneys, or hanging rabbits up by their feet.
- Severing or irritating certain nerves.
- Injecting rabbits with adrenalin.
- Injecting rabbits with a multitude of toxic factors, including digitalin, strophanthin, adonidin, ergotin, theocin, barium chloride, hydrastin, nicotine, caffeine, formalin, ergosterol, and various salts of acids and heavy metals.
- Injection of diphtheria toxin and many other bacteria cultures or bacterial byproducts.
Most of these methods caused substantial damage to the arteries and resulted in a "regenerative thickening" of one or another type. So the response-to-injury concept is quite real.
Atherosclerosis is Just One Type of Arteriosclerosis
None of these methods, however, produced anything resembling human atherosclerosis. While arteriosclerosis refers to hardening and degeneration of the arteries in general, atherosclerosis is a specific type of arteriosclerosis in which a plaque rich in lipid-loaded white blood cells, cholesterol, fatty acids, calcium, various debris — called an atheroma — invades the innermost layer of the blood vessel wall called the intima, just behind the one-cell-thick layer called the endothelium. If you are not familiar with the anatomy of a blood vessel, you can see a diagram of it here.
The research in Anitschkov’s day suggested that, while various types of arteriosclerosis occurred in humans, atherosclerosis was a much more important cause of death. Anitschkov thus concerned his research with what caused atherosclerosis.
The mechanical injuries to blood vessels or nerves produced a local repair process that involved the proliferation of cells, their congregation around the damaged area, and a resultant thickening of the vessel wall. The results were local rather than systemic, however, and never produced a lesion resembling an atheroma.
Injections of adrenalin produced much more interesting changes that were much more relevant to humans. They produced necrosis (death) of cells in the media followed by extensive calcification. A similar process was observed in some of the blood pressure experiments and in many of the experiments involving injections of metallic, bacterial, or other toxins. These changes, however, were fundamentally different from atherosclerosis, which occurs in the intima.
Medial Calcification and the Vitamin K2 Connection
That does not mean this research is irrelevant. Humans experience this type of medial calcification in diabetes, kidney disease, and aging. It appears to assault the media of arteries and the valves of the heart together. It increases arterial stiffness and decreases the artery’s ability to accomodate moderately high levels of blood pressure. One of the most important factors in this type of calcification appears to be vitamin K2.
Vitamin K-dependent proteins protect against cell death, help clear away the debris that cells leave behind when they do die, and protect against the calcification of soft tissues. In the absence of sufficient vitamin K, these proteins are deformed and fail to work properly. It appears that vitamin K2, found in animal fats and fermented foods, is far more important in this respect than vitamin K1, found in green plant foods. I have written extensively on this subject and argued that vitamin K2 is the "activator X" of Weston Price in my article, On the Trail of the Elusive X Factor: Vitamin K2 Revealed.
Despite the research in Anitschkov’s day suggesting that only atherosclerosis had major clinical importance, research in our own day shows that calcification of the media and valves is critically important to, at a minimum, the 324 million people worldwide who will be diabetic come 2025. For the US population born in 2000, the estimated lifetime risk of type 2 diabetes is one in three.2 In type 2 diabetics, medial calcification increases the risk of mortality from heart disease, stroke, and all causes. It also predicts the incidence of heart disease and stroke, including events that do not produce fatalities, and predicts the likelihood that peripheral artery disease will require limb amputation.3
So the response-to-injury hypothesis has a solid basis of evidence for arteriosclerosis of the media, and this is clinically important — but what causes atheroma, that is, the fatty plaque that causes raised lesions in the intima of the blood vessels?
To answer this question, we must look to the cholesterol-fed rabbit.
The Cholesterol-Fed Rabbit Controversy
In 1909, a researcher at the Military Medical Academy in St. Petersburg named Ignatowski produced atherosclerosis in rabbits by feeding them a diet of meat, eggs, and milk. He was pursuing a hypothesis put forward by Nobel Prize-winning microbiologist I. Metchnikov that dietary protein accelerated aging.4
In 1913, Anitschkov and his partner Chalatov were studying at the same academy and were assigned to follow up Ignatowski’s work. They progressively narrowed down the causative factor to cholesterol by feeding different foods and fractions of foods, finally producing the diease by feeding pure cholesterol dissolved in sunflower oil.4
Rabbits fed sunflower oil alone did not develop atherosclerosis. In the cholesterol-fed rabbits, however, lesions developed that exhibited a remarkable similarity to the human disease. They began as fatty streaks in the intima; circulating white blood cells then invaded the intima and engulfed the cholesterol and fat deposited there, eventually growing into large phagocytic cells that Anitschkov called xanthoma cells and we now call foam cells; eventually the developing plaque protruded into the intima in the form of a raised lesion. The lesion possessed a fatty core rich in crystalized and calcified cholesterol deposits and was covered with a fibrous cap.1
The lesions did not appear everywhere equally, but occurred in specific areas. They were most prominent in the aorta and other large arteries, especially in the areas of the artery wall that experience disturbed blood flow such as the points where the arteries branch. While they did not occur in exactly the same places as human atherosclerotic lesions, the pattern was largely similar and the underlying physiological principle dictating the location of the lesions — mainly the type of blood flow experienced by the artery wall — was the same.1
The rabbits developed cholesterol deposits all throughout their bodies, in their eyes and internal organs. Anitschkov produced a more mild form of the disease, however, by feeding the rabbits milk. In these experiments, the rabbits received a much more moderate amount of cholesterol over a much longer period of time and the resulting disease was much more focused in the arteries.1
One curious difference between rabbits and humans is that when rabbits develop atherosclerosis, their plaques never rupture and they never get heart attacks. The main determinant of plaque rupture according to the current scientific literature is the balance between collagen degradation and collagen synthesis.5 Collagen synthesis requires vitamin C. Most animals, including rabbits, make their own vitamin C, but humans do not.
Atherosclerosis itself probably diminishes the quality of life in many different ways by impeding blood flow and blood vessel function, but it clearly does not inexorably lead to heart attacks. The reason why atherosclerosis produces heart attacks in humans and not rabbits or many other animals might be that humans cannot produce their own vitamin C.
Cholesterol in the Blood, Not the Food
Anitschkov argued against calling cholesterol "the cause" of atherosclerosis, but he considered cholesterol the primary causal factor and the necessary causal factor. Mechanical injuries, adrenalin injections, and other methods used to induce various types of arteriosclerosis would accelerate the development of atheroma when they were combined with cholesterol-feeding, but they would never result in human-like atherosclerosis by themselves.
Anitschkov never concluded from his experiments that cholesterol in the diet caused atherosclerosis in humans, however. To the contrary, he wrote the following:
[I]n human atherosclerosis the conditions are different. It is quite certain that such large quantities of cholesterin are not ingested with the ordinary food. In human patients we have probably to deal with a primary disturbance of the cholesterin metabolism, which may lead to atherosclerosis even if the hypercholesterinemia is less pronounced, provided only that it is of long duration and associated with other injurious factors.
Cholesterol skeptics often argue that the rabbit is irrelevant to the human because it is an herbivore. Cholesterol-feeding has failed to produce atherosclerosis in many other species. This is true, but it misses the point. In the species where cholesterol-feeding alone does not produce atherosclerosis, the blood level of cholesterol does not rise as much as in rabbits. But in all of these species when the level of cholesterol in the blood rises high enough, atherosclerosis ensues. For example, feeding dogs cholesterol alone does not produce atherosclerosis because they turn the cholesterol into bile acids; but inhibiting thyroid hormone stops them from making this conversion, and when combined with cholesterol-feeding, it induces atherosclerosis.
As Steinberg points out, raising blood levels of cholesterol has produced atherosclerosis in baboons, cats, chickens, chimpanzees, dogs, goats, guinea pigs, hamsters, monkeys, mice, parrots, pigs, pigeons, rabbits and rats.
The role of blood cholesterol in human heart disease was supported by research showing that people with a disorder that would eventually be called familial hypercholesterolemia had dramatically increased blood levels of cholesterol and, in youth and middle age, dramatically increased relative risks of heart disease and atherosclerosis. But what caused their high cholesterol levels, and did those levels cause the atherosclerosis, and if so, did this phenomenon have any relevance to the rest of us?
And, if cholesterol was somehow the culprit in all of this, was it merely its concentration in the blood that was at play, or was something very different going on?
Lessons From Familial Hypercholesterolemia
Familial hypercholesterolemia (FH) bears a striking resemblance to the cholesterol-fed rabbit model. In mild cases, it produces earlier and more rapidly developing atherosclerosis compared to the general population. In its severe cases, it results in cholesterol deposits all throughout the body, especially in the liver, kidneys, and eyelids.4
In the mid-1970s, Brown and Goldstein discovered that FH resulted from a single genetic defect in the LDL receptor that made the cells unable to absorb LDL from the bloodstream. Steinberg argues that, since cells jealously guard their cholesterol concentrations by adjusting their synthesis of cholesterol as needed, this showed that FH patients differed from the general population in only one single way: the concentration of cholesterol in their blood.4
The finding drew several more parallels between FH and Anitschkov’s cholesterol-fed rabbits. Anitschkov argued that it was not the mere feeding of cholesterol to the rabbits that produced atherosclerosis, but the overwhelming of their capacity to use and dispose of that cholesterol. FH cells could absorb free cholesterol, but not cholesterol from LDL. Anitschkov’s rabbits developed atherosclerosis when they ate cholesterol, but not when they were injected with it — in which case it would not be packaged into lipoproteins such as LDL, which contain many other substances besides cholesterol. Looking backward, it appears that the common thread running through each model was that the level of LDL in the blood exceeded the capacity of the LDL receptors to move that LDL from the blood to the cells.
The LDL receptor highway was blocked, and the LDL traffic was jammed.
Is Steinberg correct, however, that this changes nothing but the concentration of LDL in the blood? Consider what happens in a traffic jam:
- The concentration of cars in the road increases.
- It takes you longer to get home.
When LDL can’t get from the blood into the cells, its concentration in the blood rises, but it also spends a longer amount of time in the blood. Why would that matter? This would become clear just several years later. At the end of the 1970s, the role of oxidative stress in heart disease would finally become clear.
The Role of Oxidized LDL in Heart Disease
Anitschkov believed that his research showed that atherosclerosis was of an infiltrative character rather than a degenerative character. He believed that cholesterol and other substances naturally permeated the endothelium in order to nourish the other layers of the blood vessels, and proceeded from there into the lymph fluid. When the blood level of cholesterol rose sufficiently, he argued, it entered the intima at a faster rate than it could exit and began to accumulate.
Anitschkov was correct that the disease was driven by an infiltration of lipid, and he was correct that the degeneration of the blood vessel wall was secondary to this infiltration. What he failed to realize, and could not have realized at the time, was that the entire process depended on the degeneration of the lipid.
The Discovery of Oxidized LDL
Beginning in 1979, investigators made a series of revolutionary discoveries revealing this degenerative process. When they incubated cells with LDL in the absence of other serum components, the cells underwent severe damage and began to die within 24 hours. Adding serum or HDL prevented the toxicity.4
In 1981, these researchers discovered that culturing endothelial cells with LDL caused dramatic changes to the LDL, making it denser, more electronegative, and giving it a dramatic ability to accumulate in white blood cells called macrophages. Macrophages are phagocytic, meaning they like to gobble up other things, and they are the precursors to the "foam cells" that populate atherosclerotic plaques. The researchers called this LDL "endothelial cell-modified LDL." Soon after, they discovered that the LDL was being "oxidatively modified" and that not only HDL but vitamin E (which HDL is rich in) prevented the effect.4
Oxidized LDL Causes Injury and Inflammation
Since those early findings, thousands of papers have now been published on the role of oxidized LDL in the development of atherosclerosis. Oxidized LDL causes endothelial cells to secrete "adhesion molecules" and "chemoattractants" that allow white blood cells called monocytes to penetrate in between the endothelial cells and stick to them in the subendothelial space where fatty streaks and atherosclerotic plaques develop.6
Oxidized LDL turns on the expression of genes in monocytes which cause them to convert into macrophages and eventually into foam cells, which makes them gobble up more and more oxidized LDL endlessly — but these macrophages use "scavenger receptors" rather than LDL receptors, so they never take up meaningful amounts of non-oxidized LDL; they only take up oxidized LDL, and it is oxidized LDL itself that initates this endless cycle.7
Oxidized LDL initiates the inflammatory process by causing foam cells to secrete molecules that attract T cells and other inflammatory cells.6 Oxidized LDL enhances the process whereby T cells, foam cells, smooth muscle cells and endothelial cells decrease collagen production and increase collagen degradation, which leads to the rupture of the fibrous plaque.5
Endothelial cells produce nitric oxide, a gas that protects LDL from oxidation, increases blood flow, decreases the adhesion of monocytes to the endothelium, and decreases blood clotting. Oxidized LDL impairs the endothelial cell’s ability to produce nitric oxide.8
In short, oxidized LDL contributes to the entire atherosclerotic process from start to finish. Writers who argue that atherosclerosis has nothing to do with lipids but is all about inflammation and response to injury must contend with the fact that oxidized LDL injures endothelial cells and causes inflammation!
Small, Dense (Pattern B) LDL and Oxidation — Which Comes First?
If it is oxidized LDL rather than LDL per se that contributes to atherosclerosis, the question arises of what causes LDL to oxidize. Since polyunsaturated fatty acids (PUFA) in the LDL membrane are the components that are most vulnerable to oxidation, excess PUFA and insufficient antioxidants would seem to be the most obvious culprits. Endothelial cells, however, secrete a number of oxidative enzymes such as myeloperoxidase and lipoxygenase. LDL is always exposed to endothelial cells in the blood, but if it makes its way into the subendothleial space where it can get stuck in a network of sugary proteins called proteoglycans, it would be exposed to them even more directly. Some researchers have therefore put forward the "response-to-retention hypothesis," wherein the LDL oxidizes in response to getting stuck in the subendothelial space.
In 1988, a case-control study showed that people with a preponderance of small, dense LDL were three times more likely to suffer from a heart attack.9 Researchers subsequently showed that the smaller and denser LDL gets, the more quickly it oxidizes when they subject it to oxidants in a test tube.10 Then the "response-to-retention" crowd jumped in on the game a few years later and showed that small, dense LDL were much more likely get stuck in test tube versions of the proteoglycan network of the subendothelial space.11
If the response-to-retention hypothesis is true, we are back to the infiltration hypothesis where the accumulation of LDL in the subendothelial space is driving the whole process because the accumulation causes the oxidation. This would be a convenient way of circumventing the enormously embarassing fact that the medical establishment has been pushing highly oxidation-prone PUFA oils for fifty years.
The question is, how are these LDL getting small and dense?
Within the response-to-retention paper, the authors stated that "with decreasing size and increasing density the LDL particles have less of the non-polar core covered with a surface monolayer made of phospholipids and cholesterol."
Where did the phospholipid membrane go?
A group working on lipoprotein (a), or Lp(a), published a paper in July of this year showing that virtually all oxidized LDL in the blood circulates attached to Lp(a). Lp(a) is essentially LDL stuck to a protein called apolipoprotein (a) or apo(a). This group showed that when oxidized LDL and apo(a) are incubated together, many of the oxidized phospholipids transfer directly to the apo(a).12 In other words, when the membrane of LDL begins to oxidize, parts of it hop right off the LDL particle. Could that explain why "less of the non-polar core" would be "covered with a surface monolayer" on some LDL particles?
When Steinberg and his coworkers first described the characteristics of "endothelial cell-modified LDL," one of the most conspicuous changes that occurred to the LDL particles was a marked increase in density.13
A 1997 study confirmed that the LDL taken from people with a preponderance of the small, dense type does indeed oxidize quicker in a test tube, but the oxidation status of the LDL was different before they subjected it to oxidation. The predominantly small, dense LDL had a higher ratio of oxidized-to-reduced coenzyme Q10 and a lower CoQ10-to-vitamin E ratio.14 Since CoQ10 is the first line of defense against LDL oxidation, this study strongly suggested that oxidation of the small, dense LDL had already started.
So here we have a chicken-and-egg question. Does small, dense LDL oxidize more rapidly in a test tube because it is small and dense, or because it is already partially oxidized, and its antioxidant defenses are already partially depleted? Is small, dense LDL more vulnerable to oxidation, or does LDL become small and dense when it becomes oxidized?
If LDL becomes small and dense through oxidation, then even if the test tube studies on its "stickiness" are correct and small, dense LDL is more likely to get stuck in the sugary protein network behind the endothelium, it is the oxidation driving the stickiness and not the stickiness driving the oxidation.
So we are back to square one wondering why the medical establishment never announed an emergency measure to put all the research dollars into discovering just how much damage it had done to everyone who followed its recommendations to use high-PUFA vegetable oils in place of saturated animal fats over the last fifty years.
Oxidized LDL and the PUFA Connection
Let us return to the traffic analogy for a moment. Why would an "LDL traffic jam," wherein the "LDL receptor highway" is blocked contribute to atherosclerosis?
The membrane of LDL contains polyunsaturated fatty acids (PUFA), which are highly vulnerable to oxidation. Cells continuously make antioxidant enzymes and other antioxidant compounds to protect their membrane PUFA. If PUFA start to oxidize, the cell ramps up its antioxidant production. When the liver packs cholesterol into a VLDL particle and secretes it into the blood (where it eventually becomes an LDL particle after delivering some of its nutrients to other tissues), it puts some antioxidants into the package. The PUFA have now left the comparative safety of the liver cell and have only a limited supply of antioxidants. When those antioxidants are used up, the PUFA begin to oxidize, and their oxidation products proceed to damage other components of the lipoprotein. When the oxidation becomes severe, the oxidized LDL winds up in a foam cell in an atherosclerotic plaque.
Let’s draw another analogy, this time to a jar of oil. If you use a jar of oil, you open it, exposing the PUFA within it to the oxygen in the air, but quickly put the cap back on and put it back in the fridge. What would happen if you opened the jar and let it sit on the table at room temperature? Over time, the limited amount of antioxidants in the oil would run out and the PUFA would begin to oxidize. The oil would go rancid.
Pumping LDL into the blood but letting it sit there circulating round and round exposed to oxidants rather than taking it into the shelter of the cell is like opening a jar of oil and leaving it on the table.
LDL taken from people who consume more PUFA, whether from vegetable oil or fish oil, oxidizes more easily in a test tube. Alpha-tocopherol, the major form of vitamin E, does not help.15
The specific components of the oxidized LDL particle that interact with the DNA of monocytes to transform them into macrophages and then into foam cells are oxidized derivatives of linoleic acid, a PUFA found in vegetable oils.16
A 2004 study from Brigham and Women’s Hospital and Harvard School of Public Health showed that in postmenopausal women, the more PUFA they ate, and to a much lesser extent the more carbohydrate they ate, the worse their atherosclerosis became over time. The more saturated fat they ate, the less their atherosclerosis progressed; in the highest intake of saturated fat, the atherosclerosis reversed over time.17
I will cover the topic of saturated fat, PUFA, and heart disease in greater detail in another article on the diet-heart hypothesis. Additionally, I have written a Special Report entitled How Essential Are the Essential Fatty Acids? that provides accurate and thoroughly researched information on the true requirement for PUFA, which is negligible for healthy adults. As part of my Special Reports series, I will be publishing a second PUFA Report later this year that will cover the benefits and dangers of consuming PUFA in amounts larger than the minimum requirements.
Shear Stress Explains the Locations of Plaques and the Benefits of Exercise
As in the cholesterol-fed rabbit, human atherosclerosis occurs in discrete plaques at specific locations. In both species, these plaques occur in locations that experience disturbed blood flow, such as the points where the arteries branch.
Anitschkov showed that the endothelium was more permeable to molecules labeled with dye at these points. Experimental vessel injuries that caused inflammatory responses made the endothelium even more permeable, but even in the absence of any treatment, the endothelium was naturally permeable in these areas.1
Sections of the arterial wall in these areas experience a lower level of shear stress than sections in other areas. Shear stress is the type of pressure that is caused by laminar blood flow, or the flow of blood parallel to the blood vessel wall. Shear stress decreases the permeability of the endothelium by stimulating the production of the proteins that form the junctions between the endothelial cells. Under levels of shear stress approximating those that exist at locations where atherosclerosis develops, easily visualizable gold particles the size of LDL particles slip right in between the endothelial cells, whereas the permeability to these particles is very low under levels of shear stress approximating those that exist where plaques do not develop.18
Shear stress also increases nitric oxide production. Nitric oxide increases blood vessel dilation and blood flow, decreases the adhesion of monocytes to the endothelium, decreases blood clotting, and prevents the oxidation of LDL.6
By increasing blood flow, exercise increases shear stress. Since the average shear stress over time seems to be the critical factor, exercise might help prevent atherosclerosis by decreasing the permeability of the endothelium and increasing nitric oxide production in those areas of the blood vessels where the resting level of shear stress is insufficient for protection.
What About Correlations with High Cholesterol?
Much of the cholesterol debate focuses on correlations with cholesterol. How strong are they? How consistent are they? Why do they show up in young people but not in old, in men more than women?
The debate really misses the point, because since the early 1980s the molecular evidence has made very clear that it is oxidized LDL that contributes to atherosclerosis.
Correlations with cholesterol are likely to be confounded by a variety of factors that simultaneously increase cholesterol levels and contribute to heart disease, like stress and inflammation. In fact, inflammation seems to increase cholesterol synthesis essentially as an accidental byproduct of activating the stress response through an enzyme called Rho. Rho slashes nitric oxide production and thus almost certainly makes a contribution to atherosclerosis. For more information on Rho activation, click here.
Researchers have only recently developed methods for testing levels of oxidized LDL. One group has developed an antibody that recognizes oxidized but not non-oxidized phospholipids. They have shown that the proportion of LDL-associated phospholipids that are oxidized is a much more impressive risk factor for heart disease than LDL, and when it is multiplied by the level of LDL, thus indicating the total concentration of oxidized phospholipids, it is even better. Its predictive value is lower in older people, but still strong.19
Why would the association decline with age? If we look at the totality of the evidence about the mechanisms of atherosclerosis, it appears that oxidized LDL is the necessary initiating factor, but that we should expect its prominence as a contributing factor to decrease over time. Atherosclerosis probably does not develop in the absence of oxidized LDL. Once it does develop, however, and once the oxidized LDL stimulates the formation of foam cells, those foam cells recruit T cells that make their own contribution to the inflammatory process. Animal experiments show that independent sources of inflammation cannot initiate atherosclerosis, but they can aggravate it or accelerate it. Vitamin C deficiency, systemic infection, stress, and many other factors likely make contributions alongside oxidized LDL to the weakening and rupture of the fibrous cap that ultimately leads to a heart attack.
Virtually everyone develops substantial atherosclerosis by the time they are old. In people with more oxidized LDL, it occurs faster, and consequently reaches an advanced stage at a younger age. Inflammation will not help rupture a plaque that does not exist, so it will be much less likely to cause a heart attack in a younger person unless that person has high levels of oxidized LDL and consequently advanced atherosclerosis. In an older population wherein most people have advanced plaques, the factors that weaken the plaque will become much more important than the factors that create the plaque.
Studying the issue is complicated by the fact that we are looking at oxidized LDL in the blood. Once LDL gets oxidized enough, presumably it will wind up in arterial plaque. If there are factors that protect circulating LDL from contact with the tissues it could harm, they could confound the association.
Finally, studies looking at cardiovascular incidence or mortality are confounded by the fact that atherosclerosis is only one type of arteriosclerosis, and arteriosclerosis is only one cause of cardiovascular disease. Medial calcification, arrhythmia, congestive heart failure, or other causes of emboli (particles that can cause vessels) may all contribute to cardiovascular events. Oxidized LDL should only, or at least primarily, correlate with those events caused by atherosclerosis.
So is the Lipid Hypothesis Correct?
So is the lipid hypothesis correct? Not in its original form. The weight of the evidence clearly supports a role for the oxidation of LDL and not the concentration of LDL in the blood in the development of atherosclerosis.
The oxidized lipid hypothesis has an enormous amount of evidence supporting it. The cholesterol-fed rabbit model was a model not merely of hypercholesterolemia but of hyper-oxidized-lipoproteinemia. Antioxidants cause major decreases in atherosclerosis in cholesterol-fed or Watanabe familial hypercholesterolemic rabbit models independent of cholesterol levels.4,20
We should not expect antioxidants to be fully capable of preventing the oxidation of LDL by themselves. As I discuss in my PUFA Report, antioxidants can stop oxidized PUFA from damaging other PUFA, but they can never fully repair the oxidized PUFA. The best they can do is convert it to a hydroxy-fatty acid, and it is the hydroxy versions of linoleic acid that have been shown to convert monocytes to foam cells!
Thus, all three of the following critical factors must be addressed:
- Increasing antioxidant status, especially coenzyme Q10, but also alpha- and gamma-tocopherol.
- Reducing PUFA intake.
- Increasing LDL receptor function to minimize the amount of time LDL spends in the bloodstream.
If concentrations of LDL rise in the blood because the LDL is not being utilized — for example, in familial hypercholesterolemia — then the LDL is exposing its vulnerable PUFA to conditions promoting oxidative stress for too long. The solution should not be to diminish cholesterol synthesis, imparing CoQ10 synthesis along with it, but to increase LDL utilization. The appropriate nutritional strategies for increasing LDL utilization desperately need to be researched.
A recent study showed that curcumin, a component of tumeric, increases the expression of the LDL receptor. This study may provide valuable clues. Thyroid hormone is important to the function of the LDL receptor, and many people likely have suboptimal thyroid status.
The irony in all of this is that there is no evidence to suggest that cholesterol is the culprit. In the rabbit, consuming large amounts of cholesterol increases the exposure of LDL membrane-associated PUFA to oxidation because it causes their translocation from the liver to the blood where they are detached from the cellular environment and less protected. In humans, eating cholesterol in the form of several eggs per day probably decreases the vulnerability of LDL to oxidation. See here.
The higher the concentration of free cholesterol within the LDL particle, the less vulnerable it is to oxidation. By contrast, the higher the concentration of cholesterol that is linked to fatty acids, called "esterified cholesterol," the more vulnerable the LDL is to oxidation.9 Esterified cholesterol primarily exists in the core of the particle. Free cholesterol primarily exists in the surface membrane where the initial oxidation takes place, so cholesterol seems to protect the PUFA from oxidation.
So, does cholesterol cause atherosclerosis? No!
But do blood lipids? Yes. Atherosclerosis is a disease in which degenerating lipids infiltrate the blood vessel wall and cause inflammation and degeneration of the local tissue once they arrive there. Solid evidence has amassed in favor of this view for the last 100 years.
Share this page: 






References
1. Anitschkow N, Experimental Arteriosclerosis in Animals. In: Cowdry EV, Arteriosclerosis: A Survey of the Problem. 1933; New York: Macmillan. pp. 271-322.
2. Cheng D. Prevalence, predisposition and prevention of type II diabetes. Nutrition & Metabolism. 2005;2:29.
3. Lehto S, Niskanen L, Suhonen M, Ronnemaa T, Laakso M. Medial Artery Calcification. A Neglected Harbinger of Cardiovascular Complications in Non-Insulin-Dependent Diabetes Mellitus. Arteriosis, Thrombosis, and Vascular Biology. 1996;16:978.
4. Steinberg D, The Cholesterol Wars: The Skeptics vs. The Preponderance of the Evidence.2000; San Diego: Academic Press.
5. Libby P. The molecular mechanisms of the thrombotic complications of atherosclerosis. J Intern Med. 2008;263(5):517-27.
6. Libby P. Inflammation and cardiovascular disease mechanisms. Am J Clin Nutr. 2006;83(suppl):456S-60S.
7. Tontonoz P, Nagy L, Alvarez JG, Thomazy VA, Evans RM. PPARgamma promotes monocyte/macrophage differentiation and uptake of oxidized LDL. Cell. 1998;93(2):241-52.
8. Laufs U, Fata VL, Plutzky J, Liao JK. Upregulation of Endotelial Nitric Oxide Synthase by HMG CoA Reductase Inhibitors. Circulation. 1998;97:1129-1135.
9. Austin MA, Breslow JL, Hennekens CH, Buring JE, Willet WC, Krauss RM. Low-density lipoprotein sublass patterns and risk of myocardial infarction. JAMA 1988;260(13):1917-21.
10. Tribble DL, Holl LG, Wood PD, Krauss RM. Variations in oxidative susceptibility among six low density lipoprotein subfractions of differing density and particle size. Atherosclerosis. 1992;93:189-99.
11. Camejo G, Hurt-Camejo E, Wiklund O, Bondjers G. Association of apo B lipoproteins with arterial proteoglycans: Pathological significance and molecular basis. Atherosclerosis 1998;139:205-222.
12. Bergmark C, Dewan A, Orsoni A, Merki E, Miller ER, Shin M-J, et al. A Novel Function of Lipoprotein (a) as a Preferential Carrier of Oxidized Phospholipids in Human Plasma. J Lipid Res. 2008 Jul 3;[Epub ahead of print]
13. Henriksen T, Mahoney EM, Steinberg D. Enhanced macrophage degradation of low density lipoprotein previously incubated with cultured endothelial cells: Recognition by receptors for acetylated low density lipoproteins. Proc Natl Acad Sci USA. 1981;78(10):6499-6503.
14. de Rijke YB, Bredie SJH, Demacker PNM, Vogelaar JM, Hak-Lemmers HLM, Stalenhoef AFH. The Redox Status of Coenzyme Q10 in Total LDL as an Indicator of In Vivo Oxidative Modification. Arteriosclerosis, Thrombosis, and Vascular Biology. 1997;17:127-133.
15. Nenseter MS, Drevon CA. Dietary polyunsaturates and peroxidation of low density lipoprotein. Curr Opin Lipidol. 1996;7(1):8-13.
16. Nagy L, Tontonoz P, Alvarez JG, Chen H, Evans RM. Oxidized LDL regulates macrophage gene expression through ligand activation of PPARgamma. Cell. 1998;93(2):229-40.
17. Mozaffarian D, Rimm EB, Herrington DM. Dietary fats, carbohydrate, and progression of coronary atherosclerosis in postmenopausal.
18. Conklin BS, Vito RP, Changyi C. Effect of Low Shear Stress on Permeability and Occludin Expression in Porcine Artery Endothelial Cells. World J Surg. 2007;31:733-43.
19. Tsimikas S, Brilakis ES, Miller ER, McConnell JP, Lennon RJ, Kornman KS, Witztum JL, Berger PB. Oxidized phospholipids, Lp(a) lipoprotein, and coronary artery disease. N Engl J Med. 2005;353(1):46-57.
20. Wang Z, Zou J, Cao K, Hsieh TC, Huang Y, Wu JM. Dealcoholized red wine containing known amounts of resveratrol suppresses atherosclerosis in hypercholesterolemic rabbits without affecting plasma lipid levels. Int J Mol Med. 2005;16(4):533-40.
Things the Food Industry Doesn’t Want You to Know
Posted: October 1, 2009 Filed under: Food and it's Impact on Our Health Leave a commentTwo nutrition experts argue that you can’t take marketing campaigns at face value
By Adam Voiland

With America’s obesity problem among kids reaching crisis proportions, even junk food makers have started to claim they want to steer children toward more healthful choices. In a study released earlier this year, the Centers for Disease Control and Prevention reported that about 32 percent of children were overweight but not obese, 16 percent were obese, and 11 percent were extremely obese. Food giant PepsiCo, for example, points out on its website that "we can play an important role in helping kids lead healthier lives by offering healthy product choices in schools." The company highlights what it considers its healthier products within various food categories through a "Smart Spot" marketing campaign that features green symbols on packaging. PepsiCo’s inclusive criteria—explained here—award spots to foods of dubious nutritional value such as Diet Pepsi, Cap’n Crunch cereal, reduced-fat Doritos, and Cheetos.
But are wellness initiatives like Smart Spot just marketing ploys? Such moves by the food industry may seem to be a step in the right direction, but ultimately makers of popular junk foods have an obligation to stockholders to encourage kids to eat more—not less—of the foods that fuel their profits, says David Ludwig, a pediatrician and the co-author of a commentary published in this week’s Journal of the American Medical Association that raises questions about whether big food companies can be trusted to help combat obesity. Ludwig and article co-author Marion Nestle, a professor of nutrition at New York University, both of whom have long histories of tracking the food industry, spoke with U.S. News and highlighted some things that junk food makers don’t want you to know about their products and how they promote them.
1. Junk food makers spend billions advertising unhealthy foods to kids.
According to the Federal Trade Commission, food makers spend some $1.6 billion annually to reach children through the traditional media as well the Internet, in-store advertising, and sweepstakes. An article published in 2006 in the Journal of Public Health Policy puts the number as high as $10 billion annually. Promotions often use cartoon characters or free giveaways to entice kids into the junk food fold. PepsiCo has pledged that it will advertise only "Smart Spot" products to children under 12.
2. The studies that food producers support tend to minimize health concerns associated with their products.
In fact, according to a review led by Ludwig of hundreds of studies that looked at the health effects of milk, juice, and soda, the likelihood of conclusions favorable to the industry was several times higher among industry-sponsored research than studies that received no industry funding. "If a study is funded by the industry, it may be closer to advertising than science," he says.
3. Junk food makers donate large sums of money to professional nutrition associations.
The American Dietetic Association, for example, accepts money from companies such as Coca-Cola, which get access to decision makers in the food and nutrition marketplace via ADA events and programs, as this release explains. As Nestle notes in her blog and discusses at length in her book Food Politics, the group even distributes nutritional fact sheets that are directly sponsored by specific industry groups. This one, for example, which is sponsored by an industry group that promotes lamb, rather unsurprisingly touts the nutritional benefits of lamb. The ADA’s reasoning: "These collaborations take place with the understanding that ADA does not support any program or message that does not correspond with ADA’s science-based healthful-eating messages and positions," according to the group’s president, dietitian Martin Yadrick. "In fact, we think it’s important for us to be at the same table with food companies because of the positive influence that we can have on them."
4. More processing means more profits, but typically makes the food less healthy.
Minimally processed foods such as fresh fruits and vegetables obviously aren’t where food companies look for profits. The big bucks stem from turning government-subsidized commodity crops—mainly corn, wheat, and soybeans—into fast foods, snack foods, and beverages. High-profit products derived from these commodity crops are generally high in calories and low in nutritional value.
5. Less-processed foods are generally more satiating than their highly processed counterparts.
Fresh apples have an abundance of fiber and nutrients that are lost when they are processed into applesauce. And the added sugar or other sweeteners increase the number of calories without necessarily making the applesauce any more filling. Apple juice, which is even more processed, has had almost all of the fiber and nutrients stripped out. This same stripping out of nutrients, says Ludwig, happens with highly refined white bread compared with stone-ground whole wheat bread.
6. Many supposedly healthy replacement foods are hardly healthier than the foods they replace.
In 2006, for example, major beverage makers agreed to remove sugary sodas from school vending machines. But the industry mounted an intense lobbying effort that persuaded lawmakers to allow sports drinks and vitamin waters that—despite their slightly healthier reputations—still can be packed with sugar and calories.
7. A health claim on the label doesn’t necessarily make a food healthy.
Health claims such as "zero trans fats" or "contains whole wheat" may create the false impression that a product is healthy when it’s not. While the claims may be true, a product is not going to benefit your kid’s health if it’s also loaded with salt and sugar or saturated fat, say, and lacks fiber or other nutrients. "These claims are calorie distracters," adds Nestle. "They make people forget about the calories." Dave DeCecco, a spokesperson for PepsiCo, counters that the intent of a labeling program such as Smart Spot is simply to help consumers pick a healthier choice within a category. "We’re not trying to tell people that a bag of Doritos is healthier than asparagus. But, if you’re buying chips, and you’re busy, and you don’t have a lot of time to read every part of the label, it’s an easy way to make a smarter choice," he says.
8. The food industry funds front groups that fight antiobesity public health initiatives.
Unless you follow politics closely, you wouldn’t necessarily realize that a group with a name like the Center for Consumer Freedom (CCF) has anything to do with the food industry. In fact,Ludwig and Nestle point out, this group lobbies aggressively against obesity-related public health campaigns—such as the one directed at removing junk food from schools—and is funded, according to the Center for Media and Democracy, primarily through donations from big food companies such as Coca-Cola, Cargill, Tyson Foods, and Wendy’s.
9. The food industry works aggressively to discredit its critics.
According to the new JAMA article, the Center for Consumer Freedom boasts that "[our strategy] is to shoot the messenger. We’ve got to attack [activists’] credibility as spokespersons." Here’s the group’s entry on Marion Nestle.
The bottom line, says Nestle, is quite simple: Kids need to eat less, include more fruits and vegetables, and limit the junk food.
What I want to tell you is to NOT buy food out of packages, if it needs are label to list all the ingredients, you don’t want it! Buy unprocessed food; meat, coconut oil, butter, eggs, vegetables…and a tiny amount of fruit. That’s it, leave the cereals, granola bars, chips, sodas, juices on the grocery shelf. Eat enough healthy fat and protein at each meal, the rest should be veggies. And include traditionally made meat stocks for calcium and iron (think soup from scratch).
I’m opening a Brothel..Read on…
Posted: September 30, 2009 Filed under: Food and it's Impact on Our Health, In The Kitchen with Millie- How To's Leave a commentYep, it’s true…I’m opening a brothel…LOL!
About a month ago I began offering beef and chicken stocks to my clients. They are an essential part of eating a traditional human diet..there is simply no other way to get the calcium you so desperately need. Since the 50’s people have stopped making stocks. All those stupid commercials for drugs like Boniva say, “when diet and exercise are not enough”….
Guess what? Diet and exercise ARE ALWAYS ENOUGH!! Period! No exceptions..

The response has been incredible, I am now making close to 15 quarts of stock each week. I offer them for pick-up each Monday evening…so let me know what you want…go to my webpage for details.. Please order by Thursday of the week before… Optimum Nutrition – Meat Stocks
I also offer raw butter, coconut milk yogurt, salad dressings and fresh mayonnaise, along with gluten free wedding cakes and desserts.
One The of the Most Ridiculous Articles on Weight Loss I’ve Read Recently….
Posted: September 22, 2009 Filed under: Food and it's Impact on Our Health 1 CommentFor the Overweight, Bad Advice by the Spoonful
By GINA KOLATA in the New York Times

Robyn Beck
And I’m making comments in red….
Two-thirds of Americans are overweight or obese. For most, research shows, neither diets nor moderate exercise brings significant long-term weight loss.
At least they get this right, “diets” don’t work…because people diet by cutting caloric intake, which in turn, cuts nutrient intake…and most people do that while lowering fat and protein intake, thinking it is healthier…it’s not….it only leads to eating carbs (fruits and veggies are 95% carbohydrates)…the body goes into starvation mode, not trusting that you are going to keep eating…and no weight loss occurs. Quite the contrary.
In Brief:
Weight control is not simply a matter of willpower. Genes help determine the body’s "set point," which is defended by the brain.
Health and Weight loss are a matter of cause and effect; our bodies react to what we are doing day to day. I was an extremely unhealthy and fat baby…and now am extremely thin and have been since I was 5 years old. I have had clients who weighed over 500 pounds and through proper nutrition took it off easily and have kept it off…and NOT through caloric restriction…but good solid traditional diet. Your bone size is a set point, it’s not going to change (unless you experience bone loss through poor nutrition)…but fat? Completely controllable through getting off empty carbs and eating enough fat6 and protein to get healthy and maintain perfect weight.
Dieting alone is rarely successful, and relapse rates are high. See above.
Moderate exercise, too, rarely results in substantive long-term weight loss, which requires intensive exercise.
And it takes burning 3500 calories to burn off one pound of body fat. I can run 10 miles at a 10 minute a mile clip and only burn about 450 top 500 calories!
Americans have been getting fatter for years, and with the increase in waistlines has come a surplus of conventional wisdom. If we could just return to traditional diets, if we just walk for 20 minutes a day, exercise gurus and government officials maintain, America’s excess pounds would slowly but surely melt away.
If we could just return to traditional diets they say! YES!!! A diet like your grandmother probably cooked…at least mine did, lots of meat, pan dripping and gravies, rich soups, eggs, lots of greens. But we also had lots of breads and sweets. But it wasn’t every day we had sweets, and when we did they were made with butter or lard (NOT Crisco!). In other words, real food.
When I say a traditional diet, I mean what is traditional for humans going back thousands of years; meat, fat, vegetables, fruits, nuts, herbs… Not stuff out of a box, nothing processed.
Scientists are less sanguine. Many of the so-called facts about obesity, they say, amount to speculation or oversimplification of the medical evidence. Diet and exercise do matter, they now know, but these environmental influences alone do not determine an individual’s weight. Body composition also is dictated by DNA and monitored by the brain. Bypassing these physical systems is not just a matter of willpower.
Body composition is fixed..in other words, I’m never going to be stocky, taller, muscular…but my weight I can control….. and so can everyone else. It’s called choices, making the choice to give up the sodas all day, cookies, cereals, sports drinks, ice cream, corn syrup, McDonalds, 750 calorie lattes, energy drinks, granola (cardboard glued together with corn syrup), granola bars (cardboard glued together with corn syrup, pressed into bars and coated with corn syrup), cheese food, cheese whiz…I could go on and on…..
More than 66 percent of Americans are overweight or obese, according to the federal Centers for Disease Control and Prevention, in Atlanta. Although the number of obese women in the United States appears to be holding steady at 33 percent, for most Americans the risk is growing. The nation’s poor diet has long been the scapegoat. There have been proposals to put warning labels on sodas like those on cigarettes. There are calls to ban junk foods from schools. New York and other cities now require restaurants to disclose calorie information on their menus.
But the notion that Americans ever ate well is suspect. In 1966, when Americans were still comparatively thin, more than two billion hamburgers already had been sold in McDonald’s restaurants, noted Dr. Barry Glassner, a sociology professor at the University of Southern California. The recent rise in obesity may have more to do with our increasingly sedentary lifestyles than with the quality of our diets.
But the notion that Americans ever ate well is suspect??? Of course we did, read on….
Here is A Brief History of Nutrition, it will let you see how we have gotten to the “diet” Madness we are at today-
Over the last 90 years we have seen a bewildering array of information on what we should eat. This information has come from any sources; the academic world, the Food and Drug Administration, countless “diet” books. When food “manufacturers” began advertising for the “food” they wanted us to buy, the whole subject became really confusing. We bought into all of it. We went from a diet based on real food which we had eaten throughout time, to breakfast cereals, cookies, candy, processed or instant food. By the 1980’s, 60% of American children’s diets were “non-food”. Manufactured foodstuff, chemicals, and preservatives. Then came fast food, transfats, out sugar intake took a major upswing. The rate of obesity began to climb.
In the mid-1900’s, the academic world, funded by the food processing industry, macronutrients (proteins, fats and carbohydrates) began to loom very large, food quality was pushed to the background and the notion that fats should be limited.
The first to attempt simple dietary guidelines were the dieticians, who came up with the Four Food Groups—meats, poultry, fish and beans; milk and cheeses; vegetables and fruits; and breads and cereals—an innocuous construct that offended no one and completely avoided making any judgments on dietary fats. Emphasis on macronutrient ratios came in with the USDA Food Guide Pyramid in 1992, which reflected the pro-grain conclusions of the McGovern Committee by giving prominence to carbohydrates and relegating animal foods to the smaller areas at the top of the pyramid. Fats and oils are mysteriously put with sweets (which are carbohydrates)—for reasons unknown except to government bureaucrats—and placed at the top of the pyramid with the admonition to "eat sparingly."
Both the US government and the American Heart Association (AHA) now preach fat restriction as the key to good health. Both recommend that less than 30 percent of dietary calories come from fat, with 15 percent from protein and the balance—up to 60 percent—from carbohydrates such as bread, pasta, rice, cereal, fruits and vegetables. (Milk products, nuts and beans are also sources of carbohydrates.)
To the average consumer, these guidelines might seem entirely reasonable.
If we take the governments recommendations on how we should eat the only way to achieve the dietary guidelines with foods that Americans enjoy eating is to drastically reduce meat and fat and pile on the carbs. If we follow this argument to its logical conclusion, we are led to one of two choices—either add lots of sugar to standard American meals or cut way back on animal foods and eat heaps of beans and pasta.
The latter course is the one advocated by extremists like Dean Ornish and John McDougal (and backed by Dr. Neil Barnard of the Physicians’ Committee for Responsible Medicine). Using logic that if a little is good, then even less is better, Ornish and McDougal promote a diet containing only 10 percent of calories as fat, a proposal that makes normal eating impossible. Even nuts are taboo on such a diet. Since beans can contain up to 25 percent protein and have less than 5 percent fat, they are given as the ideal protein source. If you want the complete protein provided by animal foods, your only choices are skim milk, egg whites and shellfish. These diets were invented by academicians, not cooks, and are too unpalatable—not to mention deficient in nutrients—to be taken seriously.
Diets high in carbohydrates and low in fat don’t stick to the ribs. Unimpeded by fats, which have the effect of slowing down digestion, carbohydrate foods flood the bloodstream and quickly raise the blood sugar. Without adequate fat in the diet, the blood sugar is likely to drop shortly thereafter, causing intense hunger and food cravings that are satisfied either by more high-carb foods—or by giving in to fats. Either way, the result is more calories. It’s no coincidence that as Americans have tried to avoid dietary fats; the rate of obesity has climbed. That’s because we’re eating too many calories, say the dieticians, wagging their fingers with disapproval. Unfortunately, only those with iron wills can eat high-carb and low-cal for any length of time. The weak-willed raid the cupboard or the refrigerator, bingeing and splurging on snack foods and sweets.
“The meals we romanticize in the past somehow leave out the reality of what people were eating,” he said. “The average meal had whole milk and ended with pie…. The typical meal had plenty of fat and calories.”
The typical meal had plenty of fat and calories.” DUH!!! Our diets are SUPPOSED to have plenty of calories (about 2000 a day) and plenty of fat (50% of our caloric intake should be from high quality, organic fat)!
“Nostalgia is going to get us nowhere,” he added.
Neither will wishful misconceptions about the efficacy of exercise. First, the federal government told Americans to exercise for half an hour a day. Then, dietary guidelines issued in 2005 changed the advice, recommending 60 to 90 minutes of moderate exercise a day. There was an uproar; many said the goal was unrealistic for Americans. But for many scientists, the more pertinent question was whether such an exercise program would really help people lose weight.
The leisurely after-dinner walk may be pleasant, and it may be better than another night parked in front of the television. But modest exercise of this sort may not do much to reduce weight, evidence suggests.
“People don’t know that a 20-minute walk burns about 100 calories,” said Dr. Madelyn Fernstrom, director of the weight-management center at the University of Pittsburgh Medical Center. “People always overestimate the calories consumed in exercise, and underestimate the calories in food they are eating.”
Exercise has little effect on weight. Don’t get me wrong, it great for a lot of things…cardio-vascular health, muscle fitness and tone, makes you happy, feels great. But to take off 1 pound of body weight you have to burn 3500 calories! Yes…that is a lot of calories. At my weight, 109 pounds, I can run 10 mph, and run for an hour and burn 791 calories in 1 hr. I am not prepared to run 3 1/2 hours a day to take off a pound of body fat…when I can eat perfect, or close to it…and just garden, practice yoga, dance a lot, hula hoop some, ride my bike when I want…and stay in great shape!
I found a site online to do check my body mass index, they say for my height, 5 ft 5, I should weight 130 pounds! Yuck, at even 5 more pounds my waistline thickens (and it’s 24 inches, the same as before I had 5 children!) and I start losing my shape….no way!!!
Tweaking the balance is far more difficult than most people imagine, said Dr. Jeffrey Friedman, an obesity researcher at Rockefeller University. The math ought to work this way: There are 3,500 calories in a pound. If you subtract 100 calories per day by walking for 20 minutes, you ought to lose a pound every 35 days. Right?
Wrong. First, it’s difficult for an individual to hold calorie intake to a precise amount from day to day. Meals at home and in restaurants vary in size and composition; the nutrition labels on purchased foods — the best guide to calorie content — are at best rough estimates. Calorie counting is therefore an imprecise art.
Second, scientists recently have come to understand that the brain exerts astonishing control over body composition and how much individuals eat. “There are physiological mechanisms that keep us from losing weight,” said Dr. Matthew W. Gilman, the director of the obesity prevention program at Harvard Medical School/Pilgrim Health Care.
Scientists now believe that each individual has a genetically determined weight range spanning perhaps 30 pounds. Those who force their weight below nature’s preassigned levels become hungrier and eat more; several studies also show that their metabolisms slow in a variety of ways as the body tries to conserve energy and regain weight. People trying to exceed their weight range face the opposite situation: eating becomes unappealing, and their metabolisms shift into high gear.
The body’s determination to maintain its composition is why a person can skip a meal, or even fast for short periods, without losing weight. It’s also why burning an extra 100 calories a day will not alter the verdict on the bathroom scales. Struggling against the brain’s innate calorie counters, even strong-willed dieters make up for calories lost on one day with a few extra bites on the next. And they never realize it. “The system operates with 99.6 percent precision,” Dr. Friedman said.
The temptations of our environment — the sedentary living, the ready supply of rich food — may not be entirely to blame for rising obesity rates. In fact, new research suggests that the environment that most strongly influences body composition may be the very first one anybody experiences: the womb.
According to several animal studies, conditions during pregnancy, including the mother’s diet, may determine how fat the offspring are as adults. Human studies have shown that women who eat little in pregnancy, surprisingly, more often have children who grow into fat adults. More than a dozen studies have found that children are more likely to be fat if their mothers smoke during pregnancy.
The research is just beginning, true, but already it has upended some hoary myths about dieting. The body establishes its optimal weight early on, perhaps even before birth, and defends it vigorously through adulthood. As a result, weight control is difficult for most of us. And obesity, the terrible new epidemic of the developed world, is almost impossible to cure.
THIS is the Best ‘They” Can Come Up With??????
They are basically saying obesity is almost impossible to cure? That is just stupidity…plain and simple. Americans eat carbs constantly, they act as if the have the “right” to eat anything they want and expect different results..the definition of neurosis!
The government and big Agra-food companies have sold us a bill of goods, that we need whole grains, that bread is healthy, that cereal is a decent breakfast, that granola bars are healthy…they are wrong; they are just feeding thier pocketbooks, growing the medical and pharmaceutical companies, the cancer “industry”, ….at YOUR expense.
In my career as a nutrition coach, spanning 26 years, I have had 2 different doctors tell me that they were not interested in teaching people to get well to the degree that I teach…that thier patients saw them an average of 7 times a year, and that paid the bills! I had one doctor in Ormond Beach get furious that I taught her best friend how to get rid of systemic yeast…in a month she was yeast free…and this doctor had been treating her for 3 years! And it was her best friend!! And this doctor was a nutritionist!
It’s not that complicated! Eat organic meat, rich meat broths for calcium and iron, healthy organic raw butter and unprocessed coconut oil, lots of low glycemic vegetables (green leafy veggies, mushrooms, onions, peppers, tomatoes) very small amounts of fruits and nuts, healthy organic grass fed or free range meats, organic eggs, small amounts of fermented foods (I make coconut milk yogurt, sauerkraut and kombucha tea).
That’s it, it’s that simple.We have NOT lost the “war” on obesity, we have simply gotten too lazy or too rushed to cook. We have gotten so spoiled by packaged foods that we are ruining our health…and our children’s health…
One The of the Most Ridiculous Articles on Weight Loss I’ve Read Recently….
Posted: September 22, 2009 Filed under: Food and it's Impact on Our Health Leave a commentFor the Overweight, Bad Advice by the Spoonful
By GINA KOLATA in the New York Times
Robyn Beck
And I’m making comments in red….
Two-thirds of Americans are overweight or obese. For most, research shows, neither diets nor moderate exercise brings significant long-term weight loss.
At least they get this right, “diets” don’t work…because people diet by cutting caloric intake, which in turn, cuts nutrient intake…and most people do that while lowering fat and protein intake, thinking it is healthier…it’s not….it only leads to eating carbs (fruits and veggies are 95% carbohydrates)…the body goes into starvation mode, not trusting that you are going to keep eating…and no weight loss occurs. Quite the contrary.
In Brief:
Weight control is not simply a matter of willpower. Genes help determine the body’s "set point," which is defended by the brain.
Health and Weight loss are a matter of cause and effect; our bodies react to what we are doing day to day. I was an extremely unhealthy and fat baby…and now am extremely thin and have been since I was 5 years old. I have had clients who weighed over 500 pounds and through proper nutrition took it off easily and have kept it off…and NOT through caloric restriction…but good solid traditional diet. Your bone size is a set point, it’s not going to change (unless you experience bone loss through poor nutrition)…but fat? Completely controllable through getting off empty carbs and eating enough fat6 and protein to get healthy and maintain perfect weight.
Dieting alone is rarely successful, and relapse rates are high. See above.
Moderate exercise, too, rarely results in substantive long-term weight loss, which requires intensive exercise.
And it takes burning 3500 calories to burn off one pound of body fat. I can run 10 miles at a 10 minute a mile clip and only burn about 450 top 500 calories!
Americans have been getting fatter for years, and with the increase in waistlines has come a surplus of conventional wisdom. If we could just return to traditional diets, if we just walk for 20 minutes a day, exercise gurus and government officials maintain, America’s excess pounds would slowly but surely melt away.
If we could just return to traditional diets they say! YES!!! A diet like your grandmother probably cooked…at least mine did, lots of meat, pan dripping and gravies, rich soups, eggs, lots of greens. But we also had lots of breads and sweets. But it wasn’t every day we had sweets, and when we did they were made with butter or lard (NOT Crisco!). In other words, real food.
When I say a traditional diet, I mean what is traditional for humans going back thousands of years; meat, fat, vegetables, fruits, nuts, herbs… Not stuff out of a box, nothing processed.
Scientists are less sanguine. Many of the so-called facts about obesity, they say, amount to speculation or oversimplification of the medical evidence. Diet and exercise do matter, they now know, but these environmental influences alone do not determine an individual’s weight. Body composition also is dictated by DNA and monitored by the brain. Bypassing these physical systems is not just a matter of willpower.
Body composition is fixed..in other words, I’m never going to be stocky, taller, muscular…but my weight I can control….. and so can everyone else. It’s called choices, making the choice to give up the sodas all day, cookies, cereals, sports drinks, ice cream, corn syrup, McDonalds, 750 calorie lattes, energy drinks, granola (cardboard glued together with corn syrup), granola bars (cardboard glued together with corn syrup, pressed into bars and coated with corn syrup), cheese food, cheese whiz…I could go on and on…..
More than 66 percent of Americans are overweight or obese, according to the federal Centers for Disease Control and Prevention, in Atlanta. Although the number of obese women in the United States appears to be holding steady at 33 percent, for most Americans the risk is growing. The nation’s poor diet has long been the scapegoat. There have been proposals to put warning labels on sodas like those on cigarettes. There are calls to ban junk foods from schools. New York and other cities now require restaurants to disclose calorie information on their menus.
But the notion that Americans ever ate well is suspect. In 1966, when Americans were still comparatively thin, more than two billion hamburgers already had been sold in McDonald’s restaurants, noted Dr. Barry Glassner, a sociology professor at the University of Southern California. The recent rise in obesity may have more to do with our increasingly sedentary lifestyles than with the quality of our diets.
But the notion that Americans ever ate well is suspect??? Of course we did, read on….
Here is A Brief History of Nutrition, it will let you see how we have gotten to the “diet” Madness we are at today-
Over the last 90 years we have seen a bewildering array of information on what we should eat. This information has come from any sources; the academic world, the Food and Drug Administration, countless “diet” books. When food “manufacturers” began advertising for the “food” they wanted us to buy, the whole subject became really confusing. We bought into all of it. We went from a diet based on real food which we had eaten throughout time, to breakfast cereals, cookies, candy, processed or instant food. By the 1980’s, 60% of American children’s diets were “non-food”. Manufactured foodstuff, chemicals, and preservatives. Then came fast food, transfats, out sugar intake took a major upswing. The rate of obesity began to climb.
In the mid-1900’s, the academic world, funded by the food processing industry, macronutrients (proteins, fats and carbohydrates) began to loom very large, food quality was pushed to the background and the notion that fats should be limited.
The first to attempt simple dietary guidelines were the dieticians, who came up with the Four Food Groups—meats, poultry, fish and beans; milk and cheeses; vegetables and fruits; and breads and cereals—an innocuous construct that offended no one and completely avoided making any judgments on dietary fats. Emphasis on macronutrient ratios came in with the USDA Food Guide Pyramid in 1992, which reflected the pro-grain conclusions of the McGovern Committee by giving prominence to carbohydrates and relegating animal foods to the smaller areas at the top of the pyramid. Fats and oils are mysteriously put with sweets (which are carbohydrates)—for reasons unknown except to government bureaucrats—and placed at the top of the pyramid with the admonition to "eat sparingly."
Both the US government and the American Heart Association (AHA) now preach fat restriction as the key to good health. Both recommend that less than 30 percent of dietary calories come from fat, with 15 percent from protein and the balance—up to 60 percent—from carbohydrates such as bread, pasta, rice, cereal, fruits and vegetables. (Milk products, nuts and beans are also sources of carbohydrates.)
To the average consumer, these guidelines might seem entirely reasonable.
If we take the governments recommendations on how we should eat the only way to achieve the dietary guidelines with foods that Americans enjoy eating is to drastically reduce meat and fat and pile on the carbs. If we follow this argument to its logical conclusion, we are led to one of two choices—either add lots of sugar to standard American meals or cut way back on animal foods and eat heaps of beans and pasta.
The latter course is the one advocated by extremists like Dean Ornish and John McDougal (and backed by Dr. Neil Barnard of the Physicians’ Committee for Responsible Medicine). Using logic that if a little is good, then even less is better, Ornish and McDougal promote a diet containing only 10 percent of calories as fat, a proposal that makes normal eating impossible. Even nuts are taboo on such a diet. Since beans can contain up to 25 percent protein and have less than 5 percent fat, they are given as the ideal protein source. If you want the complete protein provided by animal foods, your only choices are skim milk, egg whites and shellfish. These diets were invented by academicians, not cooks, and are too unpalatable—not to mention deficient in nutrients—to be taken seriously.
Diets high in carbohydrates and low in fat don’t stick to the ribs. Unimpeded by fats, which have the effect of slowing down digestion, carbohydrate foods flood the bloodstream and quickly raise the blood sugar. Without adequate fat in the diet, the blood sugar is likely to drop shortly thereafter, causing intense hunger and food cravings that are satisfied either by more high-carb foods—or by giving in to fats. Either way, the result is more calories. It’s no coincidence that as Americans have tried to avoid dietary fats; the rate of obesity has climbed. That’s because we’re eating too many calories, say the dieticians, wagging their fingers with disapproval. Unfortunately, only those with iron wills can eat high-carb and low-cal for any length of time. The weak-willed raid the cupboard or the refrigerator, bingeing and splurging on snack foods and sweets.
“The meals we romanticize in the past somehow leave out the reality of what people were eating,” he said. “The average meal had whole milk and ended with pie…. The typical meal had plenty of fat and calories.”
The typical meal had plenty of fat and calories.” DUH!!! Our diets are SUPPOSED to have plenty of calories (about 2000 a day) and plenty of fat (50% of our caloric intake should be from high quality, organic fat)!
“Nostalgia is going to get us nowhere,” he added.
Neither will wishful misconceptions about the efficacy of exercise. First, the federal government told Americans to exercise for half an hour a day. Then, dietary guidelines issued in 2005 changed the advice, recommending 60 to 90 minutes of moderate exercise a day. There was an uproar; many said the goal was unrealistic for Americans. But for many scientists, the more pertinent question was whether such an exercise program would really help people lose weight.
The leisurely after-dinner walk may be pleasant, and it may be better than another night parked in front of the television. But modest exercise of this sort may not do much to reduce weight, evidence suggests.
“People don’t know that a 20-minute walk burns about 100 calories,” said Dr. Madelyn Fernstrom, director of the weight-management center at the University of Pittsburgh Medical Center. “People always overestimate the calories consumed in exercise, and underestimate the calories in food they are eating.”
Exercise has little effect on weight. Don’t get me wrong, it great for a lot of things…cardio-vascular health, muscle fitness and tone, makes you happy, feels great. But to take off 1 pound of body weight you have to burn 3500 calories! Yes…that is a lot of calories. At my weight, 109 pounds, I can run 10 mph, and run for an hour and burn 791 calories in 1 hr. I am not prepared to run 3 1/2 hours a day to take off a pound of body fat…when I can eat perfect, or close to it…and just garden, practice yoga, dance a lot, hula hoop some, ride my bike when I want…and stay in great shape!
I found a site online to do check my body mass index, they say for my height, 5 ft 5, I should weight 130 pounds! Yuck, at even 5 more pounds my waistline thickens (and it’s 24 inches, the same as before I had 5 children!) and I start losing my shape….no way!!!
Tweaking the balance is far more difficult than most people imagine, said Dr. Jeffrey Friedman, an obesity researcher at Rockefeller University. The math ought to work this way: There are 3,500 calories in a pound. If you subtract 100 calories per day by walking for 20 minutes, you ought to lose a pound every 35 days. Right?
Wrong. First, it’s difficult for an individual to hold calorie intake to a precise amount from day to day. Meals at home and in restaurants vary in size and composition; the nutrition labels on purchased foods — the best guide to calorie content — are at best rough estimates. Calorie counting is therefore an imprecise art.
Second, scientists recently have come to understand that the brain exerts astonishing control over body composition and how much individuals eat. “There are physiological mechanisms that keep us from losing weight,” said Dr. Matthew W. Gilman, the director of the obesity prevention program at Harvard Medical School/Pilgrim Health Care.
Scientists now believe that each individual has a genetically determined weight range spanning perhaps 30 pounds. Those who force their weight below nature’s preassigned levels become hungrier and eat more; several studies also show that their metabolisms slow in a variety of ways as the body tries to conserve energy and regain weight. People trying to exceed their weight range face the opposite situation: eating becomes unappealing, and their metabolisms shift into high gear.
The body’s determination to maintain its composition is why a person can skip a meal, or even fast for short periods, without losing weight. It’s also why burning an extra 100 calories a day will not alter the verdict on the bathroom scales. Struggling against the brain’s innate calorie counters, even strong-willed dieters make up for calories lost on one day with a few extra bites on the next. And they never realize it. “The system operates with 99.6 percent precision,” Dr. Friedman said.
The temptations of our environment — the sedentary living, the ready supply of rich food — may not be entirely to blame for rising obesity rates. In fact, new research suggests that the environment that most strongly influences body composition may be the very first one anybody experiences: the womb.
According to several animal studies, conditions during pregnancy, including the mother’s diet, may determine how fat the offspring are as adults. Human studies have shown that women who eat little in pregnancy, surprisingly, more often have children who grow into fat adults. More than a dozen studies have found that children are more likely to be fat if their mothers smoke during pregnancy.
The research is just beginning, true, but already it has upended some hoary myths about dieting. The body establishes its optimal weight early on, perhaps even before birth, and defends it vigorously through adulthood. As a result, weight control is difficult for most of us. And obesity, the terrible new epidemic of the developed world, is almost impossible to cure.
THIS is the Best ‘They” Can Come Up With??????
They are basically saying obesity is almost impossible to cure? That is just stupidity…plain and simple. Americans eat carbs constantly, they act as if the have the “right” to eat anything they want and expect different results..the definition of neurosis!
The government and big Agra-food companies have sold us a bill of goods, that we need whole grains, that bread is healthy, that cereal is a decent breakfast, that granola bars are healthy…they are wrong; they are just feeding thier pocketbooks, growing the medical and pharmaceutical companies, the cancer “industry”, ….at YOUR expense.
In my career as a nutrition coach, spanning 26 years, I have had 2 different doctors tell me that they were not interested in teaching people to get well to the degree that I teach…that thier patients saw them an average of 7 times a year, and that paid the bills! I had one doctor in Ormond Beach get furious that I taught her best friend how to get rid of systemic yeast…in a month she was yeast free…and this doctor had been treating her for 3 years! And it was her best friend!! And this doctor was a nutritionist!
It’s not that complicated! Eat organic meat, rich meat broths for calcium and iron, healthy organic raw butter and unprocessed coconut oil, lots of low glycemic vegetables (green leafy veggies, mushrooms, onions, peppers, tomatoes) very small amounts of fruits and nuts, healthy organic grass fed or free range meats, organic eggs, small amounts of fermented foods (I make coconut milk yogurt, sauerkraut and kombucha tea).
That’s it, it’s that simple.We have NOT lost the “war” on obesity, we have simply gotten too lazy or too rushed to cook. We have gotten so spoiled by packaged foods that we are ruining our health…and our children’s health…
Those Green Produce Saver Bags ARE Plastic and NOT Biodegradable
Posted: September 18, 2009 Filed under: Food and it's Impact on Our Health 2 CommentsI have been wondering, and have done a lot of looking around to try to find the answer, but my here at Fake Plastic Fish came through, she found out the dirt on those green plastic produce bags that keep produce fresher longer.
 Sorry to go all Charlton Heston on you. It’s just that, based on several blog posts I’ve read, a lot of people seem to think that Evert Fresh green produce bags are plastic-free, and they are absolutely not. After calling the company several times a week for over a month to try to reach the owner, Lynn Everts, I finally received the information I needed today from his assistant, Tyra. She told me that the bags are indeed made from low density polyethylene (the same type of plastic in disposable grocery bags) combined with a special clay called oya which helps to keep produce fresher longer.
Sorry to go all Charlton Heston on you. It’s just that, based on several blog posts I’ve read, a lot of people seem to think that Evert Fresh green produce bags are plastic-free, and they are absolutely not. After calling the company several times a week for over a month to try to reach the owner, Lynn Everts, I finally received the information I needed today from his assistant, Tyra. She told me that the bags are indeed made from low density polyethylene (the same type of plastic in disposable grocery bags) combined with a special clay called oya which helps to keep produce fresher longer.
I have no doubt that these bags work. But I find it ironic that we would choose to purchase an ultimately disposable plastic bag (these bags can be reused up to 8 times) made from a material that lasts forever in the environment in order to preserve something that is completely biodegradable. Personally, I’d rather buy my produce more often and be careful to eat it in a timely manner than purchase brand new virgin plastic bags to make it last a little longer. And I’d rather compost the few produce items that do go bad than landfill plastic bags.
Others may feel that saving produce is worth the plastic. And that’s their choice. My problem is that folks who believe they are avoiding plastic may be purchasing these bags because of the way they are described on various web sites. On Amazon.com, two sellers, Greenfeet and 877myjuicer, list them as being made from "non-petroleum based materials," while seller, Showcase, claims they are "made from all-natural, environmentally safe materials." These claims are simply not true, and I have e-mailed Amazon to find out how to go about getting the descriptions changed.
It’s one thing for Amazon to be selling plastic bags, but it’s quite another for Reusablebags.com to promote and sell them. No where in Reusablebags.com’s description of these bags is it revealed that the base material is actually plastic. The write-up only states that the "active ingredient is a natural mineral" and further down the page proceeds to describe the mineral as a clay called "oya" which absorbs ethylene gas given off by produce as it matures. Since Reusablebags.com is a site devoted to eliminating plastic bag waste, it would be natural for a customer to assume the Evert Fresh bags were not plastic. So I’ve also e-mailed Reusablebags.com to request they update their description of this product so that their customers can make informed purchasing decisions.
Representatives from both Reusablebags.com and Evert Fresh have told me that the bags are recyclable. However, reps from neither company could provide the names of recyclers or recycling programs that would accept them. So I checked with three of my recycling insiders, and all three felt that the clay used in the bags to keep the produce fresh actually makes them a contaminant in the waste stream rather than a recoverable material. They would probably be weeded out and landfilled by plastic bag recyclers.
So, how do we keep produce fresh without plastic? It’s a good question, and I don’t have all the answers. At the farmer’s market where I table with Green Sangha, we distribute organic cotton Eco Bags, which can keep many fruits and vegetables fresh in the refrigerator if dampened. However, this past Sunday, a customer told me she’d not had good luck with loose leaf salad greens. The cloth bag couldn’t do as good a job as plastic. Any suggestions from plastic-free salad eaters?
Another customer asked me about carrots, and I did have the answer to that one! Carrots last a really, really long time if you keep them immersed in a container of water in the fridge. I like to replace the water every few days. I think this works for celery, too.
We keep apples, pears, and citrus loose in the refrigerator without any bag or container. Tomatoes and avocados stay out on the counter. Bananas stay out on the counter too but tend to turn brown pretty fast. Most other vegetables and fruits are in the dampened cotton bags in the refrigerator.
So, what are your tips for keeping produce fresh? The clay sounds like a good idea. Too bad it’s attached to a bunch of plastic. Hmmm..I wonder if it’s possible to get this clay somewhere…I’ll look into it….
Are you looking for the "9" when you buy produce?
Posted: September 18, 2009 Filed under: Food and it's Impact on Our Health Leave a commentSeptember 2, 2009
The 4 or 5-digit number that you’ll find on the little sticker on your produce is a Price Look-Up, or PLU, code. They’ve been used by grocery stores for about 20 years to identify produce for pricing at the cash register. (I always did wonder how grocery clerks could spot the difference between Bosc and Bartlett pears on sight.) These days, the International Federation for Produce Standards (IFPS), a voluntary organization of those associated with the fresh produce industry, coordinates the use of standardized codes throughout the world.
PLU codes are used for fruits and vegetables sold individually and for other items like nuts and dried fruit sold in bulk. (You won’t see a PLU code on anything with a fixed weight, like a pint of blueberries, or that’s been processed, like a fruit salad or juice.) The code signals to the retailer the information needed to determine the price – so “4131” indicates not only the type of fruit (“apple”) but also the variety (“Fuji”) and even the size (“extra large”). If you’re a produce nerd like me, you can even look up the exact variety of what you’re eating on the IFPS website.
Organic & GMO
As you’re no doubt well aware, organic or not factors into the price of what you’re buying. As a result, the IFPS decided that organic produce would be identified with a “9” in front of the standard 4 digits traditionally used for the fruit or veggie. So if that big Fuji is organic, the code won’t just be “4131” but “94131.”
Similarly, an “8” as the first of a five-digit code indicates genetically-modified produce. If that Fuji was created using GM technology, the code would be “84131.”
Retailer Codes, not Regulations
Keep in mind that these codes are administered by a voluntary organization (the International Federation for Produce Standards) that’s made up largely of produce trade associations. Their main purpose is not to inform consumers but to facilitate grocery transactions.
Produce advertised as organic must comply with the standards of the USDA National Organic Program, but there are no labeling requirements for genetically-modified foods. No need to get too worried about looking for number 8’s, though: given current technology, there is very little PLU-coded produce that would have been genetically engineered. Thought there’s plenty of GMO corn and soybeans out there, GM technology hasn’t yet made inroads on the individually-sold fruits and veggies like tomatoes, apples, etc.
The awesome image (that was) above is by Artist Cheri Kopp; see more of her work at- http://www.cherikopp.com/index.html She wanted me to take it down, but you should check out her work…


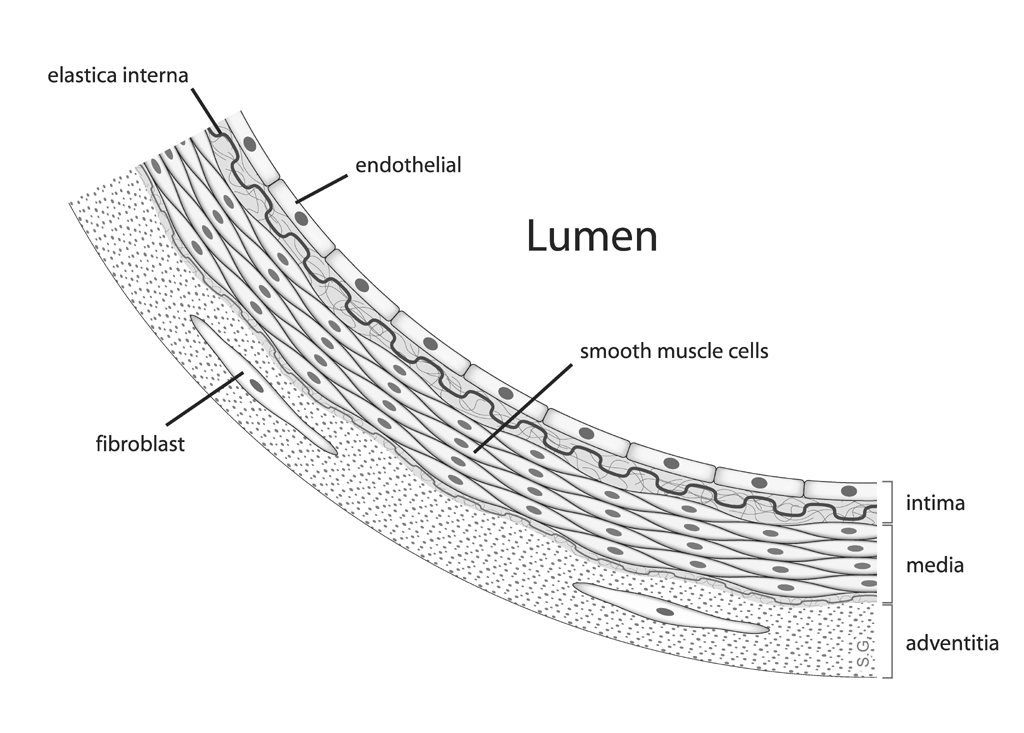{kind=link}